What Actually Moves the Needle for Male Fertility?

What Actually Moves the Needle for Male Fertility?
Men trying to improve fertility often gravitate towards supplements first. CoQ10, antioxidants, fish oil, carnitine, zinc, selenium — the list keeps growing. But across the evidence, the biggest drivers of sperm health often sit much lower in the pyramid.
While supplements may play a role in some situations, meaningful improvements in male fertility usually come from addressing broader disruptors, improving the environment sperm develop within, and identifying clinically important underlying issues.
After covering nutrition, sleep, alcohol, antioxidants, weight, testing, and lifestyle factors across this series, it’s worth stepping back and asking a simpler question:
What actually moves the needle?
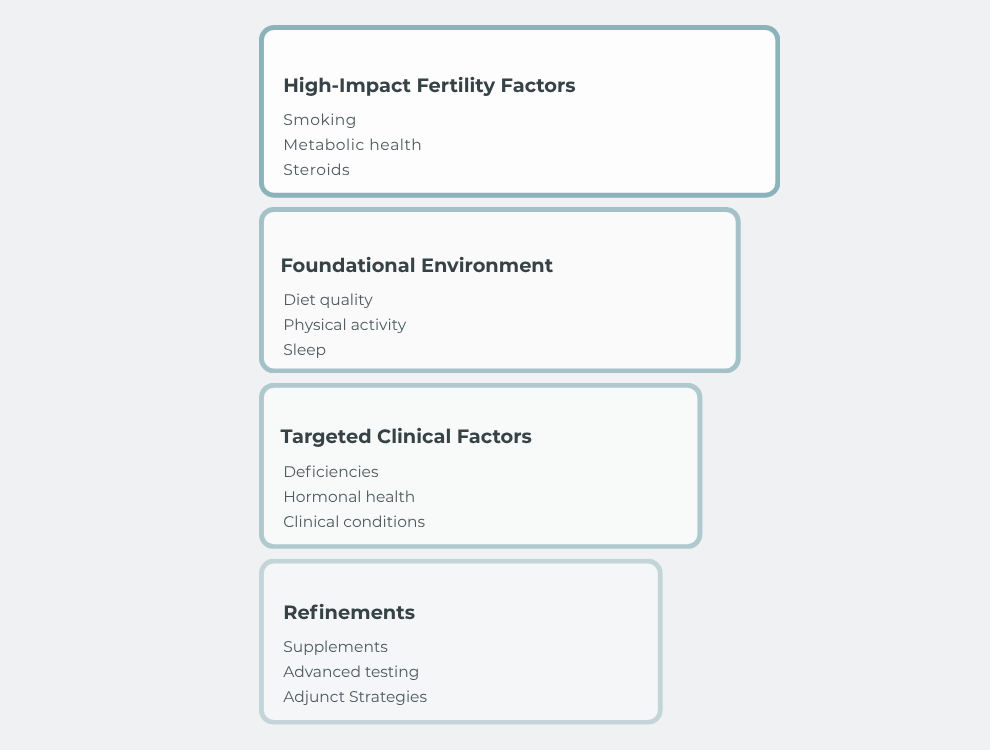
Axis Dietetics Evidence-Informed Male Fertility Framework showing where meaningful clinical leverage in male fertility tends to sit. The framework prioritises major fertility disruptors such as smoking, metabolic health, and anabolic steroid use at the foundation, followed by broader lifestyle and environmental factors including diet quality, sleep, and physical activity. Higher levels include targeted clinical assessment for underlying medical or hormonal issues, with supplements and advanced fertility strategies positioned as later refinements rather than primary foundations.
High-Leverage Fertility Factors Often Sit Lower in the Pyramid
Many men naturally focus on optimisation first — supplements, specific foods, advanced testing, or increasingly detailed fertility routines.
But some of the strongest and most consistent disruptors of male reproductive health are often broader systemic factors that can significantly influence the hormonal, inflammatory, and metabolic environment sperm develop within.
Modern male fertility guidelines increasingly emphasise broader lifestyle, metabolic, hormonal, and medical contributors rather than viewing fertility purely through the lens of supplements or isolated semen parameters (WHO; EAU; AUA/ASRM).
This does not mean every man needs to become “perfect” before trying to conceive. But it does mean that addressing major physiological disruption often provides more meaningful leverage than chasing increasingly complex refinements too early.
Smoking and Sperm Health
Smoking remains one of the clearest and most consistent disruptors of male reproductive health. Cigarette smoke exposes sperm to oxidative stress, inflammation, and DNA damage, while also affecting vascular function and the broader reproductive environment sperm develop within (Kovac et al.).
Smoking has also been associated with poorer semen parameters and higher sperm DNA fragmentation across many studies, although the degree of impact varies between individuals (Kovac et al.).
Importantly, smoking rarely exists in isolation. It often overlaps with broader lifestyle and metabolic factors that may compound reproductive stress over time.
Why Metabolic Health Matters for Male Fertility
Metabolic health likely plays a much larger role in male fertility than many men realise.
Insulin resistance, chronic inflammation, poor sleep, excess visceral fat, reduced physical activity, and sleep apnoea can all influence the hormonal and metabolic environment sperm develop within. These factors often overlap and compound one another rather than acting in isolation.
Importantly, this is not simply about body weight or appearance. Some men with obesity maintain relatively good metabolic health, while some leaner men experience significant metabolic dysfunction.
Systematic reviews and interventional studies suggest obesity and metabolic dysfunction may negatively influence male reproductive health, while improvements in metabolic health and weight loss may improve semen parameters in some men, particularly where obesity is present (Peel et al.; Andersen et al.).
Steroids, Testosterone, and Fertility Suppression
Anabolic steroids and exogenous testosterone are among the clearest examples of a major fertility disruptor overwhelming smaller optimisation efforts elsewhere.
Many men understandably associate testosterone with masculinity, performance, energy, and sexual health. But sperm production depends on a very specific hormonal signalling pathway between the brain and testes. When external testosterone or anabolic-androgenic steroids are introduced, this signalling can become suppressed, sometimes dramatically reducing sperm production (AUA/ASRM; JHRS Systematic Review and Meta-analysis).
In some men, sperm counts may fall to very low levels during use. Recovery can occur after cessation, but recovery timelines vary considerably and may take months or longer depending on factors such as duration of use, dose, and baseline reproductive health (JHRS Systematic Review and Meta-analysis).
This is an important example of why male fertility should be viewed through a broader physiological lens rather than purely as a supplement or optimisation issue.
Recreational drug use may also negatively influence male reproductive health through hormonal, vascular, oxidative stress, and behavioural pathways, although evidence quality varies considerably across substances and patterns of use.
Diet Quality and Sperm Health
Diet quality likely influences male fertility through multiple overlapping pathways including inflammation, oxidative stress, metabolic health, vascular function, and micronutrient adequacy.
Rather than focusing on individual “fertility foods,” the broader dietary pattern appears to matter more. Dietary patterns rich in whole foods, plant diversity, seafood, legumes, unsaturated fats, and minimally processed foods tend to be associated with more favourable reproductive health markers in observational research (Salas-Huetos et al.).
Importantly, this does not mean there is one perfect fertility diet. Human nutrition research is complex, and semen analysis outcomes do not always translate neatly into fertility outcomes. But overall dietary quality still appears to form an important part of the broader reproductive environment sperm develop within.
This is also where many men likely gain more leverage than they realise. Improving overall dietary quality may simultaneously influence metabolic health, inflammation, cardiovascular health, micronutrient intake, and body composition rather than targeting a single pathway in isolation.
Sleep, Recovery, and Hormonal Health
Sleep is one of the most overlooked parts of male reproductive health.
Sperm development is influenced by broader hormonal, metabolic, and circadian processes occurring across weeks to months. Poor sleep, shift work, chronic sleep restriction, and obstructive sleep apnoea may all influence this environment through effects on testosterone production, insulin sensitivity, inflammation, recovery, and oxidative stress (Hvidt et al.; Leproult & Van Cauter).
Importantly, sleep often overlaps with other major drivers rather than acting in isolation. Men experiencing poor sleep may also experience reduced physical activity, poorer dietary habits, weight gain, disrupted circadian rhythm, and worsening metabolic health over time.
This is one reason fertility rarely comes down to a single nutrient or supplement. The broader physiological environment matters.
That does not mean every imperfect night of sleep harms fertility. But consistently poor sleep and recovery may contribute to a less favourable reproductive environment over time.
Physical Activity and Metabolic Function
Physical activity likely supports male reproductive health through broader metabolic and physiological pathways rather than purely “fertility-specific” mechanisms.
Sedentary behaviour has been associated with poorer metabolic health, lower testosterone levels, erectile dysfunction, and reduced sperm viability, while regular moderate physical activity may support insulin sensitivity, cardiovascular health, inflammation control, sleep quality, and overall metabolic function (Belladelli et al.).
Importantly, more is not always better. Extremely high training loads, chronic under-fuelling, excessive endurance exercise, or overtraining may negatively affect hormonal and reproductive function in some situations (Belladelli et al.).
For most men, the goal is probably not “optimal fertility training,” but maintaining a sustainable level of regular physical activity that supports broader physiological and metabolic health over time.
Alcohol, Heat, and Environmental Exposures
Alcohol likely exists on a spectrum rather than as a simple “good” or “bad” fertility behaviour.
Heavy intake and binge drinking patterns appear more consistently associated with poorer reproductive health outcomes, while evidence around lower levels of intake remains more mixed and context dependent (Ricci et al.).
Heat exposure may also influence sperm production in some situations. Prolonged exposure to high temperatures, such as frequent hot tubs, saunas, occupational heat exposure, or prolonged laptop heat exposure, may negatively affect the testicular environment, although effects vary considerably between individuals and exposure patterns.
Environmental exposures such as air pollution and endocrine-disrupting chemicals have also attracted growing interest within male fertility research. While some evidence suggests these exposures may influence reproductive health, exposure assessment and interpretation remain challenging, and evidence quality varies considerably across different compounds and exposure levels.
Overall, these factors are best viewed as part of the broader reproductive environment rather than isolated “fertility hacks” or single causes of infertility.
Some Men Need Targeted Clinical Assessment
Not all fertility issues sit within lifestyle alone.
While improving the broader reproductive environment can be valuable, some men also have underlying medical, hormonal, structural, or genetic factors contributing to impaired fertility. In these situations, identifying the underlying issue may provide more meaningful leverage than simply adding further supplements or dietary changes.
This is one reason fertility assessment matters, particularly where there are abnormal semen parameters, recurrent pregnancy loss, prolonged difficulty conceiving, known medical conditions, previous anabolic steroid use, or symptoms suggesting hormonal dysfunction.
Importantly, this does not mean every man requires extensive testing. But it does mean fertility should not always be approached as purely a lifestyle optimisation project.
Many factors affecting male fertility, such as varicocele, endocrine disorders, genetic conditions, severe sperm abnormalities, or medication-related issues, may require assessment and management by fertility specialists, GPs, endocrinologists, or urologists rather than lifestyle intervention alone.
Varicocele, Hormones, and Underlying Medical Conditions
Some causes of male infertility are more structural or medical than lifestyle-based.
Varicocele, which involves enlargement of the veins surrounding the testes, is one of the most common identifiable findings in male infertility assessment. In some men it may contribute to impaired sperm production, oxidative stress, elevated scrotal temperature, or sperm DNA damage, although not every varicocele causes fertility problems (EAU; AUA/ASRM).
Hormonal disorders may also influence fertility through disruption of the hypothalamic-pituitary-gonadal axis and broader reproductive signalling pathways. Symptoms such as reduced libido, erectile dysfunction, fatigue, reduced morning erections, or significant changes in body composition may sometimes warrant further medical assessment (AUA/ASRM).
Underlying medical conditions such as diabetes, coeliac disease, thyroid disorders, inflammatory disease, infections, or medication effects may also contribute to impaired reproductive health in some situations.
Importantly, not every fertility issue can be corrected through nutrition or lifestyle change alone. In some cases, identifying and appropriately managing the underlying medical issue may provide the most meaningful leverage.
Supplements Usually Sit Higher Up the Pyramid
This is where many men understandably focus first.
Supplements are heavily marketed within the fertility space, and some do show potential to improve certain semen parameters in some situations. But across the evidence, supplements generally appear to function more as refinements to the broader reproductive environment rather than replacements for unstable foundations.
This is one reason supplement research in male fertility often appears inconsistent. Men entering studies may differ substantially in diet quality, metabolic health, smoking status, sleep quality, alcohol intake, obesity, underlying medical conditions, semen quality, oxidative stress burden, and baseline nutrient status. A supplement is being layered onto very different physiological environments.
Some supplements, such as CoQ10, omega-3 fatty acids, carnitine, or zinc in deficiency states, may have a reasonable rationale in selected situations. But broad antioxidant “stacks” and high-dose multi-supplement approaches often have more mixed and uncertain evidence than marketing claims suggest.
Importantly, improvements in semen parameters do not always translate into meaningful improvements in pregnancy or live birth outcomes. This distinction matters, because statistical improvement on a semen analysis is not necessarily the same thing as clinically meaningful fertility improvement.
Large reviews and trials examining antioxidants in male fertility have produced mixed findings, with substantial heterogeneity across interventions, populations, and outcomes (de Ligny et al.; Steiner et al.).
A large supplement stack layered onto unstable foundations is usually not the highest-yield strategy.
In many cases, supplements are best viewed as targeted refinements layered onto an already improving reproductive environment rather than as rescue missions sitting at the foundation of fertility care.
Why Context Matters in Male Fertility
One of the biggest problems in fertility nutrition is the search for universal answers.
Men are often told to take the same supplements, follow the same routines, or avoid the same foods regardless of their underlying health, fertility history, semen analysis findings, or broader physiological context. But male fertility is rarely that simple.
A lean, physically active man with a varicocele may require a very different approach to a man with obesity, sleep apnoea, insulin resistance, and poor dietary quality. A man recovering from anabolic steroid use presents a very different situation again. Some men may have largely unexplained infertility despite appearing otherwise healthy, while others may have clear metabolic, hormonal, or structural contributors.
Fertility outcomes are also influenced by female reproductive factors, timing, age, and broader couple-level context, which further reinforces why universal “fertility formulas” rarely exist.
This is one reason fertility should not be approached as a checklist of isolated “fertility boosters.” Context matters.
It is also why semen analysis alone does not always tell the full story. Some men with relatively normal semen parameters may still experience impaired fertility, while others with abnormal results may still conceive naturally. Fertility exists within a broader biological and clinical context rather than being defined by a single number in isolation (WHO; AUA/ASRM).
The goal is not to chase perfection across every possible fertility variable. The goal is to identify the factors most likely to be meaningfully influencing the reproductive environment in a given situation, then focus effort where the potential leverage is greatest.
Focus on Leverage, Not Just Optimisation
Male fertility is rarely shaped by one nutrient, one supplement, or one “fertility superfood” in isolation.
Sperm develop within a broader physiological environment influenced by metabolism, sleep, inflammation, hormonal signalling, diet quality, physical activity, environmental exposures, and overall health across time. Some factors appear to exert much greater influence than others, which is why understanding leverage matters.
For many men, meaningful improvements may come from addressing broader disruptors first, improving the foundational environment sperm develop within, identifying clinically important underlying issues where appropriate, and only then considering more targeted refinements.
That does not mean fertility can always be controlled. Fertility outcomes are complex, and even well-designed interventions cannot guarantee conception or pregnancy. But men often have far more influence over the reproductive environment than they realise.
The goal is not perfection.
The goal is to improve the environment sperm develop within and shift the odds in a more favourable direction.
Need Help Identifying What Actually Matters?
At Axis Dietetics, I work with men and couples across Australia to identify the factors most likely to be influencing sperm health and fertility potential.
This may include reviewing:
dietary patterns
metabolic health
lifestyle factors
sleep and recovery
supplement use
medical history
semen analysis results
broader reproductive health context
In some situations, targeted supplementation may form part of the plan. In others, the greatest leverage may come from improving broader metabolic, nutritional, or lifestyle foundations first.
The goal is to identify where meaningful leverage may actually exist and build a practical, evidence-informed plan around it.
Want to see what a fertility-supportive dietary pattern can look like in practice? You can also download the free 7-Day Men’s Fertility Meal Plan here.
Disclaimer
This article is intended for general educational purposes only and should not be considered personalised medical or nutrition advice. Male fertility is complex, and individual assessment may be important in some situations. Always discuss medical concerns, testing, supplements, or treatment decisions with your doctor or qualified healthcare professional.
References
World Health Organization. WHO laboratory manual for the examination and processing of human semen. 6th ed. Geneva: World Health Organization; 2021.
Brannigan RE, et al. Updates to male infertility: AUA/ASRM guideline. J Urol. 2024.
European Association of Urology. EAU Guidelines on Sexual and Reproductive Health. Arnhem: European Association of Urology; 2024.
Kovac JR, Khanna A, Lipshultz LI. The effects of cigarette smoking on male fertility. Postgrad Med. 2015;127(3):338-341.
Peel A, Lyons H, Tully CA, Vincent AD, Jesudason D, Wittert G, et al. The effect of obesity interventions on male fertility: a systematic review and meta-analysis. Hum Reprod Update. 2026;32(2):154-180.
Andersen E, Juhl CR, Tjønneland EM, Lundgren JR, Janus C, Dehestani Y, et al. Sperm count is increased by diet-induced weight loss and maintained by exercise or GLP-1 analogue treatment: a randomized controlled trial. Hum Reprod. 2022;37(7):1414-1422.
Mulawkar PM, Maheshwari PN, Gauhar V, Agrawal SG, Mohammed TO, Singh AG, Tak GR, Shah US, Shukla DP, Mamankar D. Use of anabolic-androgenic steroids and male fertility: a systematic review and meta-analysis. J Hum Reprod Sci. 2023;16(4):268-285.
Salas-Huetos A, Bulló M, Salas-Salvadó J. Dietary patterns, foods and nutrients in male fertility parameters and fecundability: a systematic review of observational studies. Hum Reprod Update. 2017;23(4):371-389.
Hvidt JEM, Knudsen UB, Ingerslev HJ, Philipsen MT, Frederiksen Y. Associations of bedtime, sleep duration, and sleep quality with semen quality in males seeking fertility treatment: a preliminary study. Basic Clin Androl. 2020;30:5.
Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011;305(21):2173-2174.
Belladelli F, Basran S, Eisenberg ML. Male fertility and physical exercise. World J Mens Health. 2023;41(3):482-488.
Ricci E, Al Beitawi S, Cipriani S, Candiani M, Chiaffarino F, Viganò P, et al. Semen quality and alcohol intake: a systematic review and meta-analysis. Reprod Biomed Online. 2017;34(1):38-47.
Steiner AZ, Hansen KR, Barnhart KT, Cedars MI, Legro RS, Diamond MP, et al. The effect of antioxidants on male factor infertility: the MOXI randomized clinical trial. Fertil Steril. 2020;113(3):552-560.e3.
de Ligny W, Smits RM, Mackenzie-Proctor R, Jordan V, Fleischer K, de Bruin JP, Showell MG. Antioxidants for male subfertility. Cochrane Database Syst Rev. 2022.